Krystyna Knypl




Arka wciąż płynie

Wszystkie pary tańczą

Poranek

Poranek

Poranek


Całus



family

Sylwester

Bocian

Tango





Poranek

Krystyna Knypl
W życiu bywa tak, że rodzice mieszkają w kraju przodków, a dzieci ruszają na emigracyjnych szlak... Gazeta dla Lekarzy, w zespole której jest kilka osób pracujących poza Polską, postanowiła, także wyruszyć na emigracyjny szlak. Oto logo emigracyjnej córki GdL.
![]()
Wkrótce podamy więcej informacji

Tak już w życiu jest, że dzieci chodzą swoimi, czasem emigracyjnymi drogami

Mają swoje trasy...

Swoje pólksiężyce

I swoje tereny zamknięte...
Krystyna Knypl
GdL 2 /2022
Krystyna Knypl
Dzięki uprzejmości biura prasowego World Economic Forum otrzymałam bezpłatny dostęp do e-book'a The Great Narrative. For a Better Future (https://www.amazon.com/Great-Narrative-Reset-Book-ebook/dp/B09PC4FQRZ), którego autorami są prof. Klaus Schwab i Thierry Malleret. Autorzy we wstępie książki stawiają trzy główne pytania: Jaka przyszłość nas czeka? Jakiej przyszłości pragniemy? Co musimy zrobić, aby ją osiągnąć? W epoce przemian, nie spotykanych dotychczas w historii ludzkości, wszyscy musimy postawić przed sobą takie pytania. Według autorów książka daje odpowiedź na pierwsze dwa i kładzie fundamenty do udzielenia odpowiedzi na trzecie pytanie.
![The Great Narrative (The Great Reset Book 2) by [Professor Dr.-Ing. Klaus Schwab, Thierry Malleret]](https://m.media-amazon.com/images/I/31eqa-XUKTL._SY346_.jpg)
Nie jesteśmy w stanie przewidzieć przyszłości. Możemy jednak wyobrazić ją sobie, a nawet zaprojektować; żaden wynik nie jest z góry ustalony i, jako kognitywne istoty ludzkie, zachowujemy zdolność do kształtowania świata, którego chcemy. Być może, co najbardziej istotne, możemy również przygotować się na przyszłość, stawiając czoła zarówno ryzyku, które możemy ograniczyć jak i tym, co nas zaskoczy - piszą autorzy książki.
Pandemia była jedną z takich
rzeczy. Wiele międzynarodowych organizacji i osób od lat ostrzegało, że
pandemia będzie miała miejsce, ale mimo to zaskoczyła większość świata.
Obecnie (w grudniu 2021 roku), prawie dwa lata od jej rozpoczęcia,
pandemia wydaje się nie mieć końca i wciąż się przedłuża. Mamy nadzieję,
że kryzys COVID-19 wkrótce się zakończy, ale czy tak się stanie? Zawsze
jest początek i koniec każdej epidemii jak powiedziała nam były
dyrektor generalny Światowej Organizacji Światowej Organizacji Zdrowia
( Margaret Chan*) ale pandemie jako zjawisko społeczne i i psychologiczne nie są epizodyczne: utrzymują się przez
lat. - czytamy we wstępie.
Krystyna Knypl
Przypisy
(*) Margaret Chan (陈冯富珍)
Krystyna Knypl
Motto:
Smoka pokonać trudno, ale starać się trzeba.
Ks. Benedykt Chmielowski Nowe Ateny
źródło: https://pl.wikipedia.org/wiki/Nowe_Ateny

Teraz dodajemy:
trola pokonać trudno, ale trzeba się starać ;)
Narrative medicine: description submitted to Gazeta dla Lekarzy by a patient:

On a typical day, I’d work from London Fulham Ambulance Station, where I had 15km with return journey on a push bike from my house. I used to swim several times a week. In general I have never had any health issues but appendectomy (1987) and cholecystectomy (2008). BMI of 25.
On April 9th, I started my shift as usual. We have had been called in the morning to Covid19 related cardiac arrest, where after an hour unsuccessful resuscitation I started to began experience elevated body temperature, by 14:00 body temperature raised to 39*C and I have been dismissed from front line duties to home. At the evening started flu-like symptoms (sinusitis, sore throat) including a high fever 39,5*C. Rest and accordingly to the UK Covid19 protocol 1g of oral paracetamol every 4 hours didn’t help .
On April 10th, I contacted my General Practitioner who advised me to drink lots of fluids, observe as well as to take paracetamol and in case of difficulties in breathing or desaturation to call ambulance or get to the nearest accident and emergency department. No any medication was prescribed. I was essentially bedridden for about 10 solid days from this point of my Covid19 journey.
On April 11th, I drove myself to one of the so called 'mobile coronavirus test centres' for general public' as for National Health Service workers was not available at this stage of pandemic. I lost sense of smell and taste at the evening.
On April 12/13th I was so weak that couldn’t get myself out of the bed, started to experience severe fever of 40,5*C and constant sensation of 'concrete slab' laying on my chest. Excruciating stabing, non radiating left hand sided chest pain and the worst sore throat I ever had. I was not able to swallow any solid food, what more I had a great difficulty to take breath in because of painful/burning feeling – like someone put my larynx and lungs on fire. My respiratory rate decreased to 12p/min(with abnormal breathing pattern manifesting in increased depth and prolonged period of time on inhalation) but I was still able to saturating 97% on air room on ease.
On April 14th, I received positive result for COVID19 and was advised to isolate myself for next 7 days.

On April 15th, I started with a dry cough, it felt like there was phlegm building up in my chest but it wasn’t coming loose yet (no productive coughing). I loaded up on soup, marmite, minimum 4 litres of fluids daily, cough drops, every 4hrs orally 1g of paracetamol (NSAD were non recommended by WHO) and throat spray but nothing seemed to help. My throat got progressively worse and worse that I was no longer able to sleep as simply breathing was extremely painful and insufficient. I started to desaturating whenever I did fall to sleep to 89% on an air room. At the same time, the dry cough was getting worse. I would cough so hard that I would vomit, being completely out of breath and get bloody noses. I spent 3 last days being able to sleep only in prone position and about 15min at a time before coughing/pain/breathlessness woke me up. Two days not being able to eat anything solid. Despite of taking regularly antypyretic, applying wet/cold towels and even taking cold showers I was unsuccessful to bring my body temperature down (continuously over 39,5*C). My partner decided to take me to Urgent Care at King's College Hospital London (day 6 of being sick) as my GP's advice was to observe and as long as I am not desaturating and I am not symptomatic to dyspnea or tachypnea on ease, I was qualified as 'stable from the clinical point of view'.
The strongest thing was a triage tool at King's College Hospital which accordingly to I didn’t meet the mandated criteria for hospitalisation. I explained all my symptoms and worries also presented with vital signs as follows: SAT.95%, HR110, RR12, TEM.39,7, BP 103/76.
Since, I was found clinically stable due to scoring zero on CRB-65 I have been dismissed to home without any further tests or seeing even senior practitioner.
On April 16th, during the night I experienced 41*C fever and spent most of the night cooling myself in a cold shower, started to be tachycardic (HR 115-127), felt sick, dizzy, extremely fatigue with severe joint and muscle pain as well as increased breathlessness. In the morning my partner contacted our polish friend who is obstetrician in UK and after short conversation she said although she is not an expert it sounds to her like it is pneumonia and prescribed Clarytromycin 500mg twice a day for 7 days course. After second dose of antibiotic my body temperature started to go down to 38-38,5*C. My heart rate decreased to 90b/min and saturation was maintained on 95% on an air room.
On April 17th, I was much better despite my throat felt like hamburger meat, and could feel how raw it was at the back of my mouth. All my vital signs started to stabilise but HR. I had no appetite at all so ended up on nutridrinks 5 times daily. I could not drink, and breathe without pain, I had a great difficulty to sleep as my back hurt so badly and I was super fatigued. I was totally depended on my partner Jaye, who I have been together for 6 years and he never watched me dead lift as I was a strong person, quite fit but in general he has never seen me so sick and down like this before, considering that he is also a medical professional (senior Theatre Advanced Nurse with anaesthetic specialisation at Imperial College NHS Trust) it has been genuinely scary and traumatising time for him to watch me struggle to swallow plain water, and wince in pain the whole time, not to mention he made himself off his work as I was unable to function on any level on my own for the past 7 days.
Because of my raised body temperature 38-38,5*C I was given after 7 days another antibiotic (Azitromycin) but it did not help much as this sort of fever stayed with me for another two weeks.
Approximately around 23rd of April I repeated test for coronavirus and still tested positive. The reason behind another test was continuously elevated body temperature, tachycardia, dry cough, cold sweats, abnormal breathing patterns (severe tachypnea on smallest exertion, orthopnea, night apnea, progressively worsening shortness of breath (3 breaths on one sentence) followed by pain and swelling in the joints as well as sharp chest pain increasing while inhaling.
On 1st of May, I attended King's College Hospital again as I developed severe sharp, stabbing, burning pain in the left side of the chest during breathing, especially when inhale. I also noticed that apart of my RR going up to 26 while mobilising, my saturation was dropping rapidly to 85% on as short as 2 minutes walk. I became dizzy and near fainting while walking. Also tachycardia changed in a character, previously I had mainly rapid pulse on exertion (walk from room to room brought up HR to 140-165) but at this stage also occasionally I manifested elevated heart beats on ease (115- 130b/min.).
1/05/2020 chest x-ray.
I have been discharged the very same evening with the diagnosis of: post covid19 syndrome??? No any medication or recommendation but paracetamol has been mentioned to me.
On May 2nd, I did third swab test towards coronvirus which still has come back as positive.
For next two weeks I tried some painkillers and get back to some sort of shape but instead on the 14th of May I started to desaturating to 94% on ease and 78% on tiniest exertion. The left hand sided chest pain worse and was excruciating with even shallow breathing, coughing, sneezing or laughing. The pain spread to the L shoulder, breathing effort increased significantly. I could not make few steps without pausing for rest so I decided to go again to the nearest A&E which happened to be King's.
I have been seen by consultant for the change, some blood test was done, x-ray and I was refused by multidisciplinary team (medical, radiology and A&E)to be given a chest CT scan. I was told that the benefits are smaller than the risk related to the obtained dose of the radiation. I got also worsening advice: when my saturation drops to 92% to get back to A&E. Official diagnosis was: post covid19 syndrome with no any changes noticed to my lungs.
On the discharge notification it is been written my saturation remained on 98% on ease and 95% while mobilising on room air. Truly, on my arrival was 93% but nobody mentioned that for an hour I was placed on 2l of oxygen and left for an hour to check if I am maintaining the levels.
Shortly after discharge I started slowly to drop oxygen levels again. I felt like I cannot find medical attention that I needed in UK. I managed to book and catch midnight ferry on the 15th from Harwich to Hook of Holland and drove to Poland as a last resort. It was complete lockdown, so only returning to the country polish citizens were able to cross the border. Meaning nobody else could drive me there. I reached Central Clinical Hospital of MSWiA in Warsaw within 12hours of driving on the 16th of May were was performed lung CT scan with no contrast.
14/05/2020 chest x-ray
ECG 14/05/2020
Discharge notification from King's dated on 14/05/2020
Translated Chest CT scan results as follow (16/05/2020): Transient areas of ground glass opacification with slightly dilated vessels peripherally in the a short inferior lobes of both lungs and in the superior lobe of the left lung. ln each of the mentioned lobes, the lesions occupy approx. 25% of the lobes volume.-/- Lymph nodes of the mediastinum and hila are not enlarged -/- The heart is not enlarged.-/- No fluid in the pleural cavities. The epigastrium within the limits of the study:-/-
I was admitted for 10 days to Infectious Diseases Hospital in Warsaw-translated discharge notification it is been presented below :
On admission the patient was complaining of increased back pain making it difficult for her to be lying down and sleeping, feeling of compression in the chest. In addition to this, reported shortness of breath, fever, dry cough.-/- A test for COVID-19 was positive on 9.04., 23.04.,.02.05.2020 -/- During the hospitalisation the patient was in good condition. She had periodical drops of SpO2, most likely related to sleep apnea - elective diagnostics to be considered. -/- Blood analysis revealed mildly increased ALT and GGTP activity, leucocytosis and granulocytosis. The abdominal ultrasound did not show any remarkable abnormalities. -/- Hydroxychloroquine, O2, vit.D was introduced, PCR test in view of COVID19 – negative on 21 and 23.05.2020.
Hydroxychloroquine happened to be a game-changer for me. After third dose, I finally was able to lay down on right lateral position and after 5 weeks of being deprived from sleep I managed to close my eyes for a whole two hours. Difficulties in breathing reduced greatly to the level that I started to walk a little bit again, no further support of O2 was required. After 6 days of taking well known malaria drug I got first in 46 days negative to coronavirus test result, two days after second one and I was discharged to home on the 26th of May 2020.
I spent June/July/August trying to regain some strength and giving in to my total exhaustion. My lungs would get tired and ache after more than 1min. walk at first, at the moment depends on a day but I can walk for more than an hour.
28/08/2020
After 3 months I have been referred for follow up chest CT scan which showed results as follow:
In comparison to the previous CT scan 16/05/2020, the transient ground glass opacities in both lungs have fully disappeared – full improvement. A nodule of 4 mm in diameter in the 6/10 segment of the right lung. Apart of that, the lung parenchyma is normally aerated. The mediastinal structures and great vessels of the chest are normal. No enlargement of the lymph nodes of the pulmonary hila and mediastinum was observed. Clear bronchi, no signs of narrowing. No signs of fluid in the pleural cavities.
05/10/2020
...Lingering effects 4 months later:
I had developed interesting case of tinnitus. I would listening to the phasing of the high-pitched frequencies in my ears with curiosity and trepidation. I would fall off a cliff into total exhaustion with seemingly no warning and have to spend a day in a bed. But slowly, with two steps forward and one and a half steps backwards, I was able to regain enough strength that I could take a walk by the sea side (7km). I still suffer from upper and lower limb moderate muscle weakness with tremors in hands and legs. Muscle spasms all over the body during the nights. Widespread bones, ligaments severe aching that can come and go including redness and swelling. Altered, odd feelings such as numbness, pins, tingling mainly in my fingers and foot but recently also neck and face. Funny enough my muscle with simple exercises instead of getting more flexible or stronger, are getting more shaky/trembling. I have days that I am lacking energy, what more my body is shaking like a jelly. Hands, ankle and knees joints stiffness. I still occasionally experience mild heart arrhythmias (HR 105-125). In July/August I had a great difficulties to climb the stairs as my heart rate was rapidly jumping to 160b/min. including crushing central chest pain and my RR increased to 30b/min. At the moment is slightly better and it is easier to walk on a stairs.
Typical redness and swelling of my joints:

Left elbow joint. Left wrist joint.
I am also still affected by left superior lung region pain situated next to heart that is getting worse on exertion and deep breathing. After exercising this pain is radiating to the left base of the lung and there is also an expansion feeling. Another annoying long term impact of the Covid19 is phlegm overproduction. Although, I am still short of breath while mobilising I am not desaturating while exerting. My lungs are still aching and my chest seems to be slightly tight. Bone-crushing fatigue was replaced by tiredness. Two weeks ago, someone showed me how to breath. It is strange experience to have learn how to do a thing that you never had to learn in the first place...

Another consequence of Covid19 in my case is a hair loss.
3/04/2020 - 01/06/2020 - 01/07/2020
Since ever I could remember, I had voluminous hair. Very strong and fast growing. Shortly after I managed to get rid off the virus (after 46 days from initial symptoms) I noticed a tiny bald spot on my scalp. In the following days my extremely thick shoulder-length hair started falling out in clumps, bunching up in the shower drain. I also observed increased hair breakage, split ends, lacklustre hair, hair roughness and weakness.
It took
so long for me to get consistent medical attention because I have been
regarded as a 'mild case' while frontline medical professionals were
busy managing an epidemic. In the matter of fact I was steadily but
progressively deteriorating in my first 5 weeks of sickness. The last
five months have taught me, over and over again, that we should trust
our instincts. My fitness continue slowly to improve with rehabilitation
at Pulmonary Hospital in Olsztyn. I caught the virus very early, and
I can't tell you how long, if ever it takes to recover from it, because
I have not recovered yet. I hope this case will help to have more
insight on possible Covid19 cases and post complications.
The story will continue...
GdL 2/2022
Alicja Barwicka M.D., Ph.D.
We all experience stress, but for most of us these situations are associated with negative emotions, so we tend not to expect them. There are, however, certain types of stress known in the literature as eustress, which have positive overtones, generating optimistic emotions and motivating to action. Since stress is always a reflection of an imbalance between the organism's capabilities and the demands of the situation caused by the stressor, the organism very quickly tries to restore this balance by taking remedial action. If fate has unexpectedly granted us the prize of 5 000 000 PLN, our mental balance has been strongly damaged, and for the organism, it is extremely strong stress. In medical terms, therefore, we are dealing with a significant disturbance of homeostasis. Such a strong stimulus quickly causes an increase in blood serum levels of adrenaline and noradrenaline, as well as free fatty acids and triglycerides. Fortunately, the situation does not last long, because such stressors enjoy our sympathy, so we quickly establish a list of people who should not be notified about winning, calculate the cost of potential purchases, and our mental balance and biochemical parameters return to baseline without leaving repercussions.
Life by scale
The concept of stress was first introduced by Hans Hugon Selye dedicating many years of work to the subject, but the greatest development of scientific research on issues related to stress and its consequences occurred in the last decades of the 20th century. In 1967, Thomas Holmes and Richard Rahe of Washington University in Seattle described an alternative concept of stress based on the concept of stressors. They developed a scale of 43 life events that were ranked according to the amount of remedial action the body needed to adapt to the stressful event. The relative strength of stressful situations was examined by assigning the stimulus a corresponding conventional value of stress units on a scale of 0 to 100. This resulted in the popular Social Readjustment Rating Scale (SRRS) questionnaire, which is still used today.
When we violate the balance ...
In this questionnaire, we can find several commonly occurring stressful situations, which can affect each of us, and the predominant ones are those with a negative emotional tinge, generating sadness, anxiety, or anger. Social Readjustment Rating Scale is such a useful tool, that to evaluate various random situations, its extended version was created, taking into account a much greater number of stressors. There are many positive situations, which should generate only joy (e.g. going on vacation). However, our body also treats them as a disturbance of balance and a challenge to be faced. So it activates its defensive forces, the pituitary gland, and adrenal glands prepare for biochemical warfare in the same way as in the case of a threat related to, for example, breaking into the house. And yet we don't mind such reactions, because we like positively stressful challenges very much indeed.
You can always change your profession
As we all know, professional matters can provide us with many stressful experiences. While a stable professional situation and lack of new tasks do not stress the pituitary-adrenal axis, change of duties or working conditions can generate stress calculated by SRRS at 29 - 36 points. If going further, we decide to completely change the profession, the stress (no matter if positive) is correspondingly even more intensified. In the history of medicine, there are many examples of physicians who earlier or later changed their profession, resigned from medical studies (Henryk Sienkiewicz), or expanded their practice by pursuing other activities, such as Tadeusz Boy-Żeleński. It was difficult for some, but not all of them found a place in history thanks to their difficult decision.
Twenty-eight or thirty-eight?
When 10 years ago Dr. Krystyna Knypl decided to start the Gazeta dla Lekarzy (Newspaper for Doctors) using her medical knowledge and rich clinical experience, she probably did not think that this decision would turn out to be so successful. At a time when every publishing house is struggling with financial difficulties and patches up "economic holes" by placing advertisements, it might seem that a magazine without advertisements cannot survive in the brutal publishing market. And here is a surprise! Not only did it survive, but it is growing in strength and power. Apart from factual texts from various fields of medicine, we find here a lot of the latest information gathered in short news-forms, always with a reference to the source material, issues from the history of medicine and the history of our medical families, as well as texts on the ills (not only professional) of the medical community. The growing number of national and international readers is not only impressive but also a constant encouragement for the editorial team to work on new issues. I think that the scoring of stress units defining situations accompanying this excellent project would require modification of the SRRS scale, as 100 points of satisfaction are not enough. For the time being, however, following the scientifically developed and still valid SRRS scale, it has to be noted that the founder and editor-in-chief of Gazeta dla Lekarzy constantly generate 28 stress units due to her "outstanding personal achievements". However, as life requires constant development, I would like to congratulate her and extend my best wishes that she continues to develop in the direction of an upward "change in financial status", if only due to her high score (38 stress units according to SRRS scale). With an active way of life and enjoying the publishing success an increase of 10 stress units should not be a problem, and every new penny would be the beginning of new "outstanding personal achievements".
In celebrating a decade of business, one must already be thinking about the next one. For the medical community, the current years are difficult. Some people are running away from their medical profession. There are, of course, objective reasons for this, but think about it, colleagues. You can always leave, but not everyone will be able to become a fulfilled publisher or a great writer.
To those who hesitate, I recommend
- First of all, become independent, because according to the SRRS scale "trouble with the boss" generates as many as 23 stress units,
- secondly - to read Gazeta dla Lekarzy (Newspaper for Doctors), which will allow us to broaden our knowledge, care for our professional dignity, and if necessary comfort us in (not only) professional hardships.
HAPPY BIRTHDAY TO YOU, GAZETA DLA LEKARZY !
https://www.youtube.com/watch?v=ZDl6oWohq7k

Alicja Barwicka
GdL 2 /2022
Krystyna Knypl
Leczenie COVID-19 jest olbrzymim wyzwaniem dla każdego lekarza oraz każdego systemu ochrony zdrowia na całym świecie. Poszukiwane są różne metody zapobiegania oraz leczenia tej choroby, jednak ich skuteczność nie jest zadawalająca zarówno w wymiarze jednostkowym, jak i globalnym. W dniu 13 stycznia 2022 na łamach Gazety dla Lekarzy przedstawiono streszczenie teoretycznego doniesienia o zastosowaniu naproksenu jako leku mającego działanie przeciwwirusowe
https://gazeta-dla-lekarzy.com/index.php/wazniejsze-nowosci/1681-naproksen-w-leczeniu-covid-19
Informacja powyższa jest streszczeniem doniesienia O.Terrier i wsp. "Antiviral properties of the NSAID drug naproxen targeting the nucleoprotein of SARS-CoV-2 coronawirus" https://www.mdpi.com/1420-3049/26/9/2593
W badaniu metodą spektoskopii fluorescencyjnej, anizotropii fluorescencyjnej oraz testów dynamicznego rozpraszania światła wykazano trwałe wiązanie naproksenu z białkiem N czyli nukleoproteiną wirusa SARS-Co-V-2. Skukiem tego jest zablokowanie funkcji białka N, a w efekcie duże ograniczenie replikacji wirusa i dzialanie przeciwzapalne poprzez hamowanie kaskady cyklooksygenazy.
Poza powyższym doniesieniem teoretycznym w toku jest badanie kliniczne "Efficacy of addition of naproxen in the treatment of critically III patients hospitalizen for COVID-19 infection (ENACOVID)" , w którego opisie znajdujemy następujące uzasadnienie do podawania naproksenu:
Choroba koronawirusowa 2019 (COVID-19) jest spowodowana zakażeniem SARS-CoV-2. Zaostrzenie odpowiedzi zapalnej u krytycznie chorych pacjentów zakażonych COVID-19 wymaga zastosowania odpowiednich terapii przeciwzapalnych w połączeniu z działaniem przeciwwirusowym. Tak więc, leki łączące działanie przeciwzapalne i przeciwwirusowe mogą zmniejszyć objawy niewydolności oddechowej wywołanej przez COVID-19. Ten podwójny efekt może jednocześnie chronić ciężko chorych pacjentów i zmniejszać wiremię, ograniczając w ten sposób rozprzestrzenianie się wirusa. Naproksen, zatwierdzony lek przeciwzapalny, jest inhibitorem zarówno cyklooksygenazy (COX-2), jak i nukleoproteiny (NP) wirusa grypy A. NP koronawirusów (CoV), jednoniciowych wirusów o dodatnim sensie, dzielą z jednoniciowymi wirusami o ujemnym sensie, takimi jak wirus grypy, zdolność wiązania się z genomowym RNA i jego ochrony poprzez tworzenie z RNA samoistnych oligomerów o strukturze helikalnej. Wykazano, że naproksen wiąże się z NP wirusa grypy A poprzez elektrostatyczne i hydrofobowe interakcje z konserwowanymi resztami rowka wiążącego RNA i C-końcowej domeny. W konsekwencji, wiązanie naproksenu konkurowało z asocjacją NP z wirusowym RNA i utrudniało proces samoasocjacji NP, co silnie ograniczało transkrypcję/replikację wirusa. Lek ten może potencjalnie wykazywać właściwości przeciwwirusowe wobec SARS-CoV-2, co sugerują prace modelowe oparte na strukturach CoV NP. Wysoka konserwacja sekwencji w obrębie rodziny koronawirusów, w tym zespołu ostrej ciężkiej niewydolności oddechowej (SARS-CoV) i obecnego koronawirusa SARS-CoV-2 pozwala na przeprowadzenie takiego porównania. Ostatnie badanie kliniczne wykazało, że połączenie klarytromycyny, naproksenu i oseltamiwiru zmniejszyło śmiertelność pacjentów hospitalizowanych z powodu infekcji grypą H3N2. Niewłaściwa odpowiedź zapalna u pacjentów z COVID-19 została wykazana w ostatnim badaniu, w którym pacjenci oddziału intensywnej terapii mieli wyższe poziomy IL2, IL7, IL10, GSCF, IP10, MCP1, MIP1A i TNF w osoczu w porównaniu z pacjentami spoza oddziału intensywnej terapii.
Sugerujemy, że naproksen mógłby połączyć szerokie spektrum działania przeciwwirusowego z dobrze znanym działaniem przeciwzapalnym, co mogłoby pomóc w zmniejszeniu ciężkiej śmiertelności związanej z COVID-19.
https://clinicaltrials.gov/ct2/show/NCT04325633
Badanie jest wykonywane we Francji, sponsorem badania jest Assistance Publique - Hôpitaux de Paris (https://www.aphp.fr/hopitaux). W badaniu bierze udział 30 pacjentów, głównym badaczem jest prof. Frédéric Adnet, kierownik oddziału intensywnej terapii L’hôpital Avicenne et du Samu de la Seine-Saint-Denis w Bobigny, we Francji.
Opis przypadku
53 letnia kobieta, lekarz pediatra pracująca w POZ, przyjmująca pacjentów z infekcjami górnych dróg oddechowych wśród których 2 -3 dziennie okazywało się mieć dodatni test w kierunku Covid -19. Grupa A Rh(+).
Wzrost:164 cm, waga 108 kg. Dg. Nadciśnienie tętnicze Io leczona z tego powodu bisocardem 5mg/dobę. RR 135/95. T68/min (w wywiadzie bigeminia komorowa), od czasu włączenia bisocardu bez zaburzeń rytmu serca. Zmiany zwyrodnieniowe na wszystkich odcinkach kręgosłupa, nasilone w odcinku lędźwiowym, dające okresowo nasilone dolegliwości bólowe. W wywiadzie przed 11 laty usunięcie czerniaka z okolicy międzyłopatkowej
Zaszczepiona trzema dawkami szczepionką Comirnaty https://www.pfizerpro.com.pl/product/comirnaty/szczepionka-mrna-przeciw-covid-19/ulotka-chpl-comirnaty miano przeciwciał anty SARS-CoV-2 3000 jednostek.
8 /01/ 2022: skargi na bóle głowy w okolicy zatok o obocznych nosa oraz bóle żeber, uczucie zatkania nosa, katar. Temperatura 36,9o . Tachykardia 120 / min. Wykonany przez pacjentkę w warunkach domowych test antygenowy dodatni.
9/01/ 2022. - nadal ból głowy oraz bóle żeber, katar, pacjentka wykonała test antygenowy, który dal wynik dodatni.W godzinach południowych samodzielnie pojechała samochodem (10 km) do laboratorium, gdzie wykonano test RT-PCR. Otrzymany w godzinach wieczornych test RT-PCR był dodatni.
Konsultacja telefoniczna z lekarzem internistą, który zaproponował przyjmowanie naproxenu. Pacjentka dysponowała w domu naproksenem a 220 mg i w związku z tym rozpoczęła przyjmowanie leku w dawce 2 x440 mg. Wieczorem przyjęła pierwszą dawkę naproksenu. Wypełniła wniosek na IKP o wykonanie testu RT-PCR. Ok 22.00 otrzymała wynik RT- PCR dodatni.
10 /01/ 2022: do wymienionych wyżej dolegliwości dołączyło się uczucie znacznego osłabienia. Mogła przejść kilka metrów do łazienki, natomiast pokonanie 12 stopni na schodach do pokoju na pierwszym piętrze było dużym wyzwaniem, na granicy możliwości.
11 /01/ 2022: Po 2 dobach przyjmowania naproksenu poczuła się znacznie lepiej – zmniejszył się katar, ustąpiły bóle głowy, mogła wykonywać drobne czynności porządkowe w domu.
13 /01/ 2022: piąta doba przyjmowania naproxenu, zmniejszyła dawkę do 2x220 mg w związku z zaobserwowanym przedłużonym krwawieniem po zadrapaniu skóry w okolicy kolana. W wywiadzie skłonność do krwawień, wielokrotnie wykonywane badania ( płytki krwi, koagulogram) prawidłowe.
14 /01/ 2022: czuje się dobrze, może wykonywać czynności domowej wymagające umiarkowanego wysiłku fizycznego, nie ma bólów ani duszności. Zmniejszyły się dolegliwości bólowe z narządu ruchu.
16 / 01 /2022. pacjentka czuje się dobrze, wykonany w dniu dzisiejszym test antygenowy jest ujemny.
Opis powyższego przypadku przedstawiono także na www.sermo.com , globalnym/amerykąńskim portalu dla lekarzy, jest on dostępny pod linkiem https://app.sermo.com/post/888866 (dostęp tylko dla zarejestrowanych lekarzy). Opis przypadku spotkał się z bardzo dużym zainteresowaniem kolegów lekarzy z całego świata.
Piśmiennictwo
1.Antiviral properties of the NSAID drug naproxen targeting the nucleoprotein of SARS-CoV-2 coronawirus" https://www.mdpi.com/1420-3049/26/9/2593
2. Efficacy of Addition of naproxen in the treatment of Critlically ill patients hospitalized for COVI-19 infection (ENACOVID)
https://clinicaltrials.gov/ct2/show/NCT04325633
3.Naproksen w ciągu godziny obniża o 82% ilość wirusów w płucach - badanie naukowe. Oprac. Ewa Bzymek
https://psnlin.pl/artykuly,naproksen-w-ciagu-godziny-obniza-o-82-ilosc-wirusow-w-plucach-badanie-naukowe,21,140.html
4.CHPL Naproxen a 220 mg
file:///C:/Users/Codzienne/AppData/Local/Temp/Ulotka-8189-20181212000000-4849_N-20181226000339.pdf

Krystyna Knypl
GdL 1 / 2022
3/02/2022. Up date - artykuł przeczytało 3727 osoby. Cieszymy się, że porusozny temat zastosowania naproksenu spotyka się z zainteresowaniem Czytelników.

Krystyna Knypl
W COVID-19 aktywność układu adrenergicznego oraz układu renina-angiotensyna-aldosteron odgrywają bardzo ważną rolę. Zwiększony poziom katecholamin aktywuje układ adrenergiczny prowadząc do aktywacji układu renina- angiotensyna-aldosteron oraz wzrostu aktywności ACE2. Stan taki sprzyja zwiększonemu wnikaniu SARS-CoV-2 do wnętrza komórek., które może grozić powikłaniami COVID-19.
W jednym z retrospektywnych wieloośrodkowych badań kohortowych oceniających wpływ kilku leków przeciwnadciśnieniowych na śmiertelność wewnątrzszpitalną w grupie COVID-19, z co najmniej 30-dniową obserwacją, wykazano, że ryzyko śmiertelności było mniejsze w przypadku stosowania antagonistów wapnią i beta-blokerów. Autorzy wysunęłi hipotezę, że działanie beta-blokerów może przeciwdziałać aktywacji układu współczulnego podczas burzy cytokinowej oraz zapobiega ciężkiemu przebiegu COVID-19.
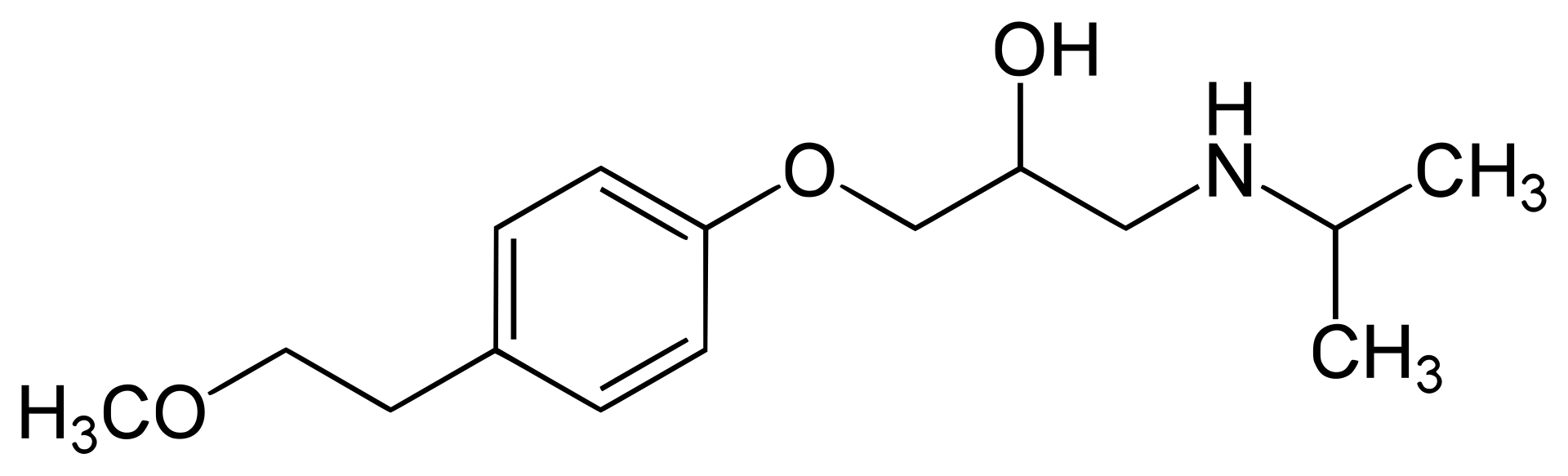
Metoprolol
Źródło informacji:https://en.wikipedia.org/wiki/Metoprolol
W innym wieloośrodkowym retrospektywnym badaniu u starszych pacjentów z grupy COVID-19 również wykazano, że stosowanie beta-blokerów wiązało się ze zmniejszeniem śmiertelności i duszności. Analiza wieloczynnikowa wykazała, że stosowanie beta-blokerów było związane z łagodniejszym przebiegiem choroby po przyjęciu.
Źródło:
Hypertension and COVID-19: Potential use of beta-blockers and a call for randomized evidence. Mochamad Yusuf Alsagaff i wsp.
https://www.sciencedirect.com/science/article/pii/S0019483221002303
Krysyna Knypl
GdL 1/2021
Krystyna Knypl
Otrzymałam akredytację prasową w European Medicines Agency (https://en.wikipedia.org/wiki/European_Medicines_Agency) i obejrzałam na żywo pierwszą w tym roku konferencję prasową na temat COVID-19. Konferencja rozpoczęła się o godzinie 16:00 i trwała około 45 miniut. W konferencji uczestniczyło około 200 dziennikarzy europejskch.
Prelegenci poinformowali, że ilość zakażeń COVID - 19 wzrasta, dotychczasowe dawki szczepionki chronią w 70 % przed hospitalizacją, dodanie dawki przypominającej zwiększa ochronę do 90 %. Ponadto przebieg zakażenia jest lżejszy u osób zaszczepionych, ale mimo to duży odsetek pacjentów wymaga hospitalizacji. W środowisku medycznym trwa dyskusja jaką wybrać najlepszą kompozycję szczepionek. W kwietniu 2022 będzie dostępna, w związku z pojawieniem się mutacji Omicron, kolejna modyfikacja szczepionki. Dziennikarze pytali jak długo będą trwaly procesy rejestracyjne zmodyfikowanej szczepionki w EMA. Odpowiedziano, że 3 do 4 miesięcy, co oznacza, że podczas wakacji można spodziewać się nowej oferty szczepionkowej.

Konferencja prasowa EMA w dniu 11 stycznia 2022 roku
Źródło: print screen z strony www na youtube
https://mail.google.com/mail/u/0/#inbox/QgrcJHsTgtSJfPVctJJMpBPzQPcKkxnXQvv?projector=1
Komentarz KK: obyśmy zdrowi byli! czego życzę wszystkim naszym Czytelnikom.
Krystyna Knypl
GdL 1 /2022
Krystyna Knypl
Istnieje pilna potrzeba specyficznego leczenia przeciwwirusowego skierowanego przeciwko SARS-CoV-2 w celu aby zapobiec najcięższym postaciom COVID-19. Poprzez zmianę przeznaczenia znanych leków o działaniu przeciwzapalnym, niedrogie terapie mogą być bardzo pomocne w leczeniu wielu pacjentów. Wycelowanie w nukleoproteinę N koronawirusa SARS-CoV-2 może być strategią hamowania replikacji wirusa i prawdopodobnie innych istotnych funkcji związanych z wirusową nukleoproteinę N. Naproksen jest zarejestrowany od 1976 roku. Właściwości przeciwwirusowe naproksenu wykazano już wcześniej wobec wirusa grypy A. w obecnym badaniu wykazano, że naproksen wiąże się z nukleoproteiną wirusa SARS-Cov-2 zgodnie z przewidywaniami modelowania molekularnego. Naproksen utrudniał rekombinowaną oligomeryzację i hamował replikację wirusa w zakażonych komórkach.

Linia komórkowa Vero pochodzi z nerki kotawca zielonosiwego, którego portret przedstawia powysza fotografia
Źródło ilustracji:https://en.wikipedia.org/wiki/Grivet
W komórkach VeroE6 i odtworzonym ludzkim pierwotnym nabłonku oddechowym modeli zakażenia SARS-CoV-2, naproksen specyficznie hamował replikację wirusa i chronił nabłonek oskrzeli przed zakażeniem. Nie wykazano hamowania replikacji wirusa paracetamolem lub inhibitorem COX-2 celekoksybem. Tak więc, spośród badanych leków z grupy niesterydowych przeciwzapalnych tylko naproksen łączył właściwości przeciwwirusowe i przeciwzapalne. Dodanie naproksenu do standardu leczenia COVID-19 może być w znaczącym stopniu korzystne.

Powyższa praca omawia pozytywne wyniki badań nad naproksenem przeprowadzonych na linii komórkowej VeroE6 (https://pl.wikipedia.org/wiki/Linia_kom%C3%B3rkowa_Vero).
Wkrótce opublikujemy na łamach GdL opis przypadku klinicznego ilustrującego korzystne wyniki leczenia u 53 letniej kobiety chorującej na Covid-19.
.Źródła:
Molecules 2021, 26, 2593. (IF = 4,411) https://www.bioxbio.com/journal/MOLECULES
https://doi.org/10.3390/molecules26092593 https://www.mdpi.com/journal/molecules
Naproksen CHPL http://leki.urpl.gov.pl/files/25_Naproxen_tab.pdf
Krystyna Knypl
GdL 1 /2022

Afiliacje autorów artykułu. Autorzy nie zgłaszają konfliktu interesów.
Krystyna Knypl Motto: Młodzi MYŚLĄ, że starzy są głupi, ale starzy WIEDZĄ, że młodzi są głupi. Agatha Christie , Morderstwo na ple...





{kind=link}